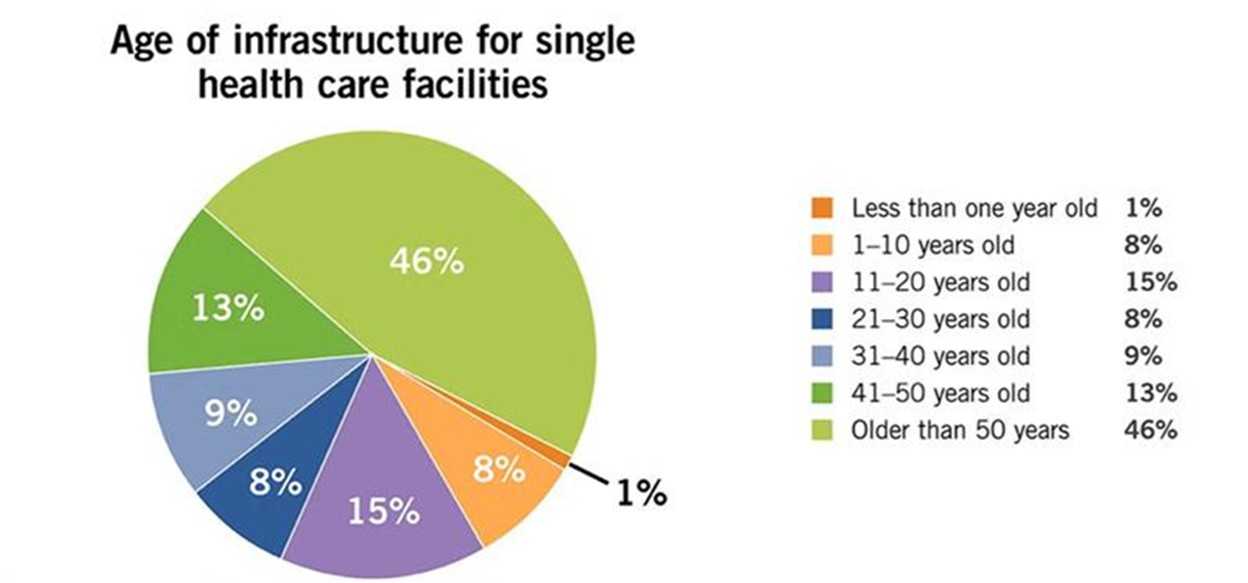
In a 2025 article in Health Facilities Management titled “Deferred maintenance and master planning,” author Mike Mochel discusses the growing need for organizations to prioritize infrastructure renewal due to building age and systems that are beyond their serviceable life.
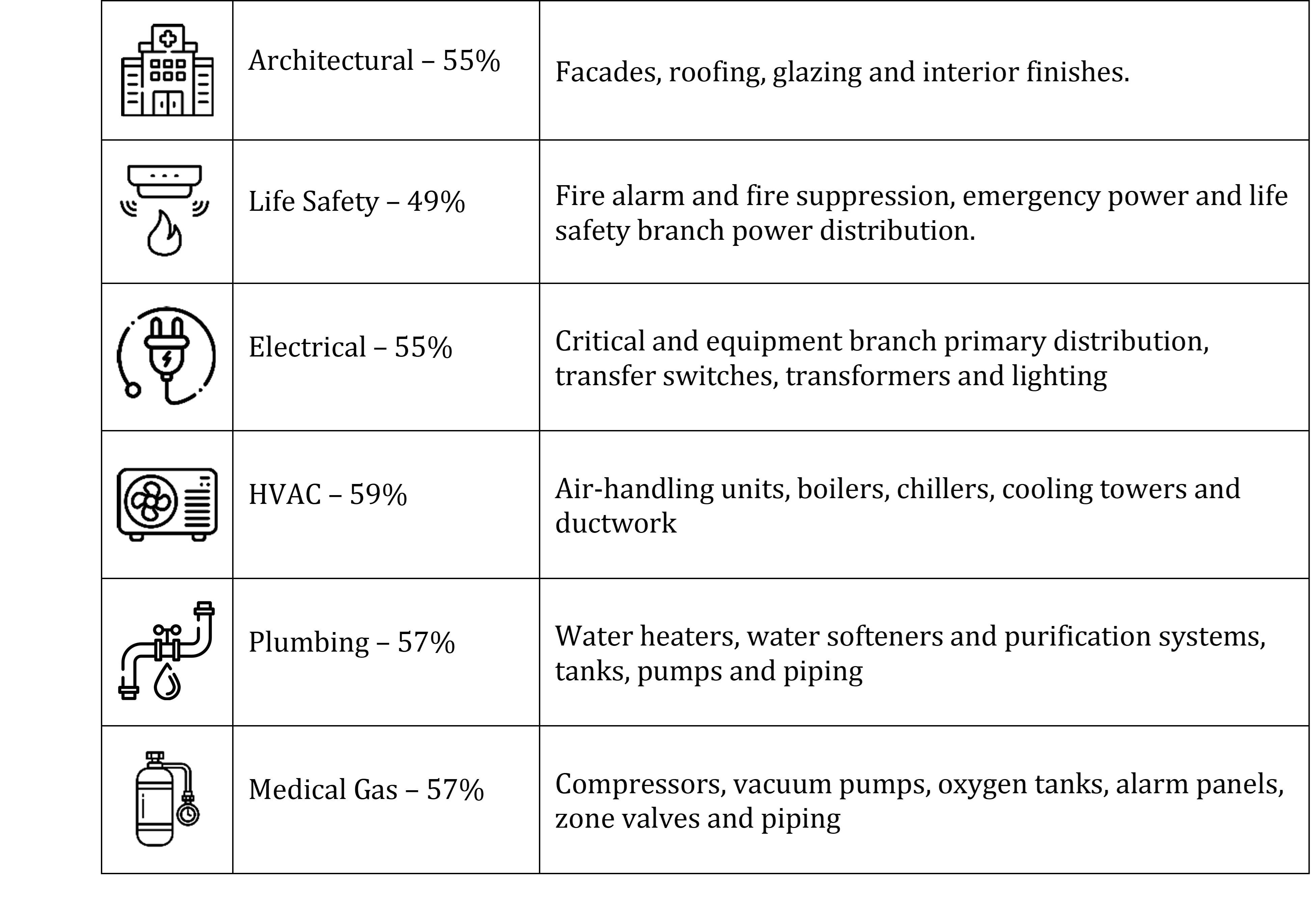
The article also shares data from the Brightly Origin National Infrastructure Benchmark Metrics, stating that in acute and non-acute healthcare infrastructure, deferred maintenance costs are over 50% for most systems (https://bit.ly/4uRaWlk) (see Table 1).
As facilities direct capital funding toward deferred maintenance, engineers must design system upgrades in occupied, fully operational buildings — work that requires careful planning to minimize disruptions to ongoing operations while maintaining safety and system reliability.
Compounding this challenge is the fact that many existing facilities were never designed to accommodate modern equipment or expanded system capacities. Engineers must often contend with undersized or poorly located mechanical rooms, which limit installation options and complicate access for both construction and future maintenance.
As a result, design teams must develop innovative solutions — such as phased implementations, creative equipment layouts, or the use of adjacent spaces — to successfully integrate upgraded systems into constrained environments.
Where to start
One way to help an organization prioritize capital funding needs is through a facility condition assessment (FCA). An FCA is a structured, data-driven evaluation of a building’s physical condition — encompassing its infrastructure systems, components and interior finishes — that helps pinpoint current deficiencies and future risks.
An FCA typically evaluates several key factors, including:
Physical condition of building systems and components;
Redundancy levels to support operational resilience;
Code compliance gaps relative to current standards;
Suitability for increased acuity or evolving operational demands;
Adaptability for future space conversion or repurposing;
Remaining useful life of critical systems and assets.
By synthesizing these elements, the FCA serves as a strategic tool to align capital planning with organizational goals, risk tolerance and long-term facility performance.
In addition to conducting infrastructure assessments, it is critical to proactively understand the potential impact of shutdowns during design, as it is often a significant factor in owner decision-making in terms of system layout. The organization’s facility team is the first step in understanding when systems, if at all, may be taken offline. Many times, in a hospital, full system shutdowns cannot be accommodated, and temporary measures may be required.

Case study No. 1
A strong example of this approach is a project currently under renovation in northern Wisconsin. The original hospital, built in 1971, includes a remote central utility plant (CUP), internal mechanical rooms and multiple small penthouses that have been added incrementally over the years to support facility expansions.
Infrastructure within the CUP includes large chillers, heating hot water boilers, incoming domestic water service, domestic water treatment systems, domestic water heaters and major electrical equipment. For a facility of its age, the plant was originally sized appropriately; however, it has reached the end of its useful life.
After evaluating the facility, the team determined that all major equipment within the plant required replacement due to age, diminished reliability and the lack of readily available parts needed to properly service the systems and maintain required capacity. These limitations not only impact ongoing maintenance efforts but also introduce operational risk to the facility.
The team coordinated meetings with the owner and the mechanical and plumbing teams to develop a detailed phasing strategy and identify locations for replacement equipment. This effort involved rethinking how space within the facility could be used to support the upgrades.
For example, by replacing aging air handling units originally located in the basement with new rooftop units, space was freed up within the existing mechanical rooms and then repurposed to house new medical gas equipment.
This allowed the new systems to be installed, commissioned and fully tested prior to tying into the existing infrastructure. As a result, the final connection to the active system was streamlined, and required only a few hours of downtime, which greatly minimized impacts to ongoing hospital operations.
During the FCA, the existing domestic water system received low scores, making it a priority for replacement. The facility was code deficient and relied on a single water service, which provided no redundancy and increased operational risk. In addition, the original galvanized piping was nearing the end of its service life and contributing to ongoing water quality concerns.
By coordinating with the local utility, civil engineer and site contractor, the project team developed a strategy to introduce a second water service into the CUP. Installing the new service first established redundancy and provided a stable platform for subsequent system upgrades, such as new water softening and water heating equipment, as well as new water mains connecting to the main hospital building through accessible utility tunnels.
The building’s heating and cooling systems required a similarly phased approach, though each presented challenges that demanded different solutions.
For the heating system, the replacement strategy focused on replacing the hot water boilers sequentially, one at a time, so the system can remain operational throughout construction. This approach provided the facility with continuous heating throughout the transition, helping to preserve environmental conditions for patient care during the process.
The chilled water system required a different strategy. Due to insufficient isolation valving within the existing system and extended equipment lead times, it was not feasible to replace components in a fully phased manner without impacting operations. To address this, a temporary chiller system is being implemented to provide the necessary cooling capacity while the permanent system upgrades are completed. This enables the existing equipment to be taken offline without disrupting facility operations.
This project demonstrates how FCA-driven prioritization, combined with strategic phasing and creative use of space, enables major system upgrades in active facilities with minimal disruption.
Case study No. 2
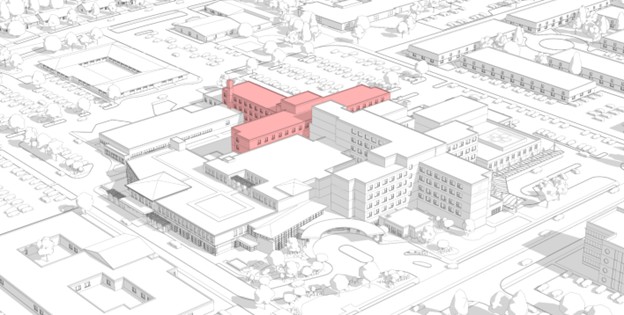
The second case study involves demolishing an existing hospital wing sandwiched between two existing buildings and constructing a new bed tower on the same footprint of the demolished building while the facility remains fully operational. The original building, constructed in 1958, is slated to come down this fall, and is nestled between the existing CUP and the rest of campus, which includes various additions to the original hospital, dating from 1979 to present.
Detailed assessments of mechanical, electrical and plumbing systems enabled the team to understand current capacities, determine if existing systems could support the new project, and identify utilities impacted by the planned demolition.
The existing 1958 building was the artery for almost all major utilities for the newer hospital sections that were to remain. As such, our team was tasked with providing the hospital with domestic water, medical gas, chilled water, steam and fire protection while the new tower was constructed.
Close collaboration with facility staff and the project team helped to identify a path that allowed construction of the new underground utility tunnel, switch over the systems, demolish the old building, and construct the new tower without impacting utilities critical for patient care. We worked to identify the new and existing loads, new utility routes and establish a phased implementation, ensuring that all aspects of the tunnel were thought through before construction started.
This project is another strong example of the growing healthcare design trend toward targeted infrastructure investment rather than full-scale replacement. In this case, it has allowed the team to deliver a modern bed tower and upgraded systems with improved facility performance, all while minimizing patient care disruptions.
It is clear from the case studies that addressing deferred maintenance in design requires more than replacement; it demands strategy, collaboration and adaptability. FCA-driven prioritization, thoughtful phasing and a strong partnership with facility teams allows designers to transform aging infrastructure into resilient, high-performing systems.
Ultimately, the success of an infrastructure renewal project is measured not just in the upgraded systems, but also by delivering the systems in a way that protects occupant safety, and positions the facility to meet future demands.
Ryan Hunwardsen, PE, ASSE 6060, is a mechanical engineer with HGA Architects and Engineers who has led the design of numerous, complex healthcare projects from concept through construction for facilities across the country, with experience in both renovation and new build projects. Specializing in plumbing and medical gas infrastructure for healthcare, Ryan works with clients to understand code compliance, sustainability, infection control and resilient system design.
Jill Imig, PE, EDAC, is vice president at the Milwaukee HGA Architects and Engineers office. She currently serves as HGA’s mechanical engineering department leader as well as a plumbing engineer for complex projects in all market sectors. Imig is a member of the American Society of Plumbing Engineers, American Society of Healthcare Engineers and the Medical Gas Professional Healthcare Organization. She has served as the past president for the ASPE Wisconsin Chapter for several terms. Imig can be reached at [email protected].
Logan Stone, PE, is a plumbing engineer in the Milwaukee office at HGA Architects and Engineers. He specializes in designing plumbing infrastructure for healthcare campuses, as well as other market sectors across the country. Stone is an active member of the American Society of Plumbing Engineers and an adjunct professor at the Milwaukee School of Engineering, where he teaches plumbing design to students majoring in architectural engineering.